
NEW STUDENT HEALTH REQUIREMENTS
Undergraduate, Graduate, and
Professional Students (Ithaca Campus)
Welcome New Students!
Cornell Health provides medical care, mental health services,
disability services, and advocacy for the wellbeing of all
students. Over 220 staff members, with a wide range of
training, expertise, and personal and professional
experiences, work together to serve our diverse student
body. Visit us when you come to campus and online at
health.cornell.edu. You’ll discover that we are focused on
supporting your health and promoting a healthy campus
community. Let us help you thrive at Cornell!
New Student Health Requirements
Cornell Health oversees the New Student Health
Requirements process, through which you will provide
information required to comply with state and federal laws,
meet public health guidelines, and support optimal health
care for you during your time at Cornell. The information you
provide, as well as all health care you receive at Cornell
Health, is confidential. Health care records are completely
separate from all other university records.
Overview
1. Print this document. It will guide you through all the steps
to meeting Cornell’s Health Requirements.
2. Plan ahead. This process involves completion of a number
of forms, and documentation of a physical examination
and immunizations.
3. Log onto myCornellHealth
with your Cornell net ID:
mycornellhealth.health.cornell.edu.
This is our secure patient portal. You will access your
Health Requirements forms there.
4. Complete all forms; submit required documentation.
View your progress at “Forms” in myCornellHealth.
* If we find problems, we will send an email alert
directing you to read a secure message at
myCornellHealth for further instructions.
5. The status on the To Do List at newstudents.cornell.edu will
be updated after a review of your materials demonstrates
compliance with immunizations and TB screening. Please
allow several weeks for review.
Deadlines
* Fall semester entrants: June 15, 2018
* Fall semester transfer students: July 31, 2018
* Spring semester entrants: December 20, 2018
Checklist for Completing Requirements
1. New Student Health History
Complete online form
2. Health Emergency Contact Information
Complete online form
3. Privacy and Consent: under age 18
Print Parent/Guardian Permissions form
Ask parent or guardian to read and sign
Upload or send completed form
Privacy and Consent: age 18 and over
Complete two online forms: Part 1 and Part 2
4. New York State Immunization Registry: under age 19
Complete online form
New York State Immunization Registry: age 19 and over
Complete online form
5. New Student Immunization and TB Screening History
Carefully review instructions (attached)
Obtain copies of your official immunization records
(from health care provider, school, or military) and any
recent TB screening test reports
Use official records to complete online form
Upload or send copies of official records
If you decide not to get the Meningococcal vaccine,
you must submit the Meningococcal waiver form
(pdf)
6. Physical Examination Form
Physical exam within the past 18 months is strongly
recommended for all incoming students
Physical exam (performed after March 1, 2018) is
required for NCAA/intercollegiate athletes
Take this form to your health care provider for
documentation of exam
Upload or send the Physical Examination Form
Other Forms You May Need to Complete
Recruited NCAA/Intercollegiate Athletes
Sports Clearance Process for Student Athletes
(pdf)
Athletes with ADD/ADHD Medical Exception Form (pdf)
Vet Students
Vet Student Medical Examination Form
(pdf)
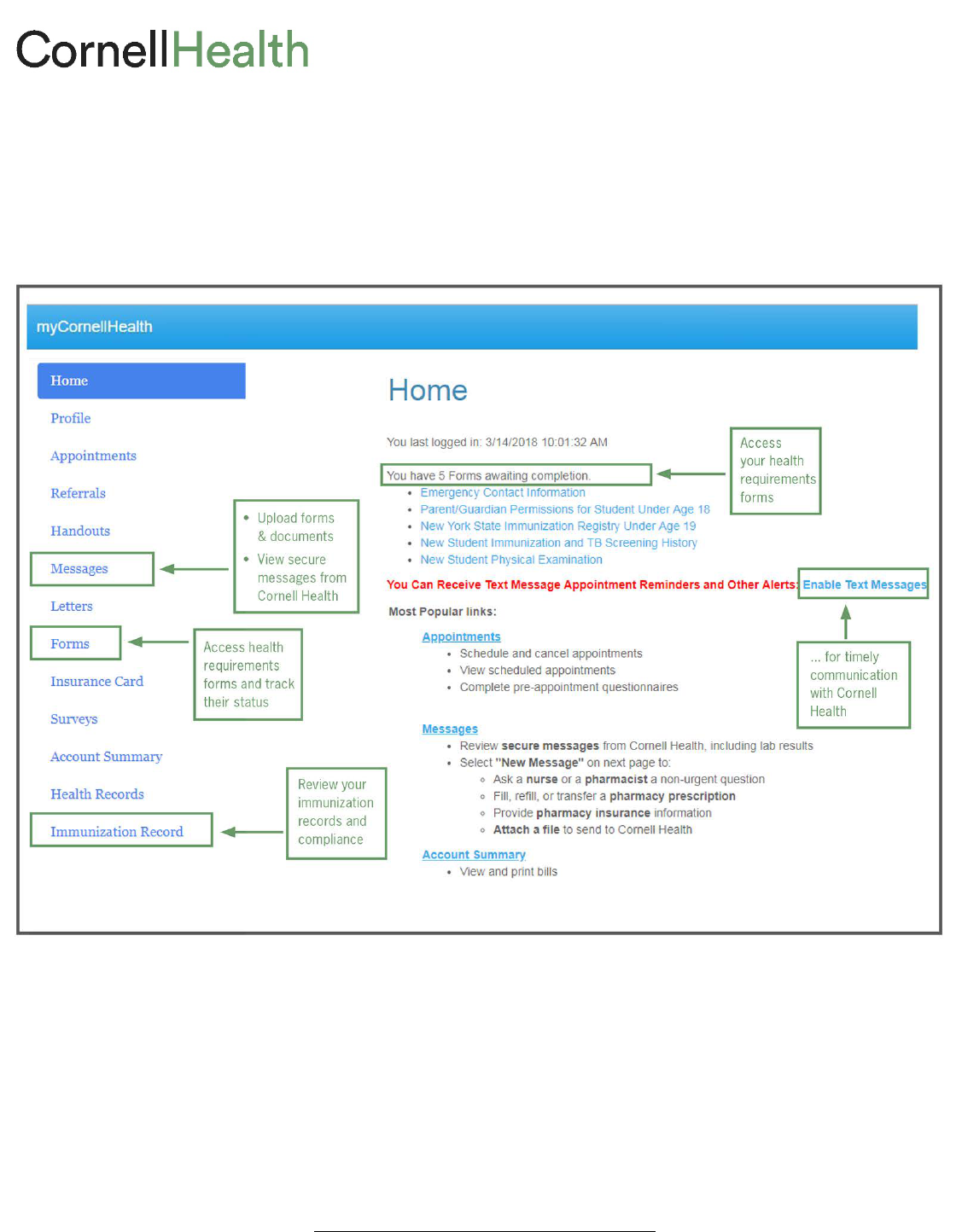
Using “myCornellHealth”
1. Access Cornell Health’s secure patient portal by going to mycornellhealth.health.cornell.edu
2. Login with your Cornell NetID and password
3. Enter your date of birth
4. Access everything you need from the Home screen
To upload forms and documents:
• Select “Messages” from navigation
• From the “Secure Messages Inbox,” select “New message”
• From the “Select Communication Option” window, select “Send a message or attachment to Health Records”
• Select “I understand” to continue
• In the “Compose New Secure Message” window:
− Identify the form or document in the “Subject” window (If a form or document has several pages, please
upload it as one multi-page document. Do not combine different forms or documents into one attachment.)
− Add attachment (.png, .gif, .jpeg, .jpg, .pdf; file size limit 4 MB)
− You may need to send several messages, depending on your requirements
To learn more about myCornellHealth: health.cornell.edu/get-care/mycornellhealth

New Student Immunization and
TB Screening INSTRUCTIONS
Who must complete this form?
• All students taking 6 or more credits in any Cornell University program must complete this form.
• If you were a full-time student at Cornell between 2012−2018: you may skip the “Required Immunizations.” You may need
to document a recent TB screening test. See “Tuberculin Screening Requirement” below. If you are not required to complete
this form, you may remove it from your form list in myCornellHealth: open the form, scroll to the bottom, click “Submit.”
Instructions
Step 1: Obtain official records from your health care provider, school, or military; or ask your health care provider to complete
the attached Cornell Health form. Records must include your full name and birthdate, and be in English.
Step 2: Go to myCornellHealth, and open the online New Student Immunization and TB Screening History form.
Step 3: Enter your immunization information (and, if required, TB screening test results) into the online form.
Step 4: Upload a copy of the printed Cornell Health immunization form or other comparable official records.
Required immunizations (Items 1 – 20)
To comply with New York State laws and public health guidelines, you must provide documentation that you have met immuni-
zation requirements for: Measles/Mumps/Rubella, Meningococcal, Tetanus/Diphtheria/Pertussis, and Varicella (Chicken Pox).
If you are not able to provide official documentation demonstrating that you have met all immunization requirements, you must
schedule (and keep) an appointment for immunizations at Cornell Health as soon as you arrive on campus. Failure to do so will
result in late fees and a hold on your registration. To schedule, call the Requirements Office: 607-255-4364.
Recommended immunizations (items 21 – 24)
We urge you to receive these vaccinations recommended by the U.S. Centers for Disease Control and Prevention and the
American College Health Association: Hepatitis A, Hepatitis B, and Human Papilloma Virus (HPV).
• Enter information about all the recommended vaccinations (and other vaccinations, Items 25 – 34) you have received.
• Provide copies of official immunization records.
• If you would like to receive recommended vaccinations after you arrive on campus, please ask when you are getting
required immunizations. If you have met all of your immunization requirements, you can call Cornell Health to schedule an
appointment for the recommended immunization(s) you want: 607-255-5155.
Tuberculin (TB) screening requirement (items 35 – 38)
Following public health and college health guidelines, Cornell requires full-time students from countries that have a “high
incidence” of tuberculosis (pdf) to provide documentation of results from a recent TB screening blood test. We recommend
testing for all students, especially those who have spent time in a country where TB is endemic.
• If you are from a country with a “high incidence” of TB, you must document your TB test here and provide copies of official
test result records.
• Please note: only Quantiferon-TB Gold or T-SPOT blood test will be accepted. Skin tests do not meet this requirement.
• If your TB test result was positive, you also must submit a chest x-ray report (no films, please).
− Students entering in the summer or fall of 2018: your test must be dated September 1, 2017 or later.
− Students entering in the spring semester of 2019: your test must be dated February 1, 2018 or later.
• If you are not able to submit documentation of an approved method of TB testing before coming to Cornell, you must
schedule (and keep) an appointment for TB screening at Cornell Health as soon as you arrive on campus. Failure to do so
will result in late fees and a hold on your registration. To schedule, call the Requirements Office: 607-255-4364.

Paying for vaccinations and TB testing at Cornell Health
• The charges for required and recommended immunizations, and for required TB screening tests, are covered by Cornell’s
Student Health Plan (SHP).
• They are not covered by Cornell’s Student Health Fee. If you have private health insurance, you will be charged for required
immunizations and TB testing. Check with your insurer to make sure you understand their reimbursement policy.
Submit official documentation
• Upload copies of your official records.
− You may do so at the end of the New Student Immunization History on myCornellHealth
, or by selecting
“Immunization Record” from the menu and choosing “Add Immunization Record.”
− Be sure to “SAVE” your work on the Immunization History before uploading records.
• If you are unable to upload records, you may either fax them to 607-255-0269, or mail them to:
CORNELL HEALTH
ATTN: Requirements Office
110 Ho Plaza
Ithaca, NY 14853-3101
PLEASE NOTE: Once submitted, review of your records may take up to three weeks. If we discover any problems, we will send an
email to your Cornell address, directing you to read a secure message at myCornellHealth. Please follow up promptly to assure
compliance with Cornell requirements and avoid late fees and registration holds.

Immunization and TB Screening
DOCUMENTATION
INSTRUCTIONS
Step 1: Ask your health care provider to complete and sign this form. NOTE: If you have comparable official records from your
health care provider, school, or military, you may submit those rather than using this printed form.
Step 2: Once you have your records, go to myCornellHealth, and open the online New Student Immunization and TB Screening History form.
Step 3: Enter your immunization information (and, if required, TB screening test results) into the online form.
Step 4: Follow instructions in the online form to upload a copy of this form OR other comparable official records.
Student name (last, first, middle)
Date of birth (mm-dd-yy) Cornell net ID #
REQUIRED IMMUNIZATIONS
Students taking 6 or more credits must provide documentation that you have met all four of these immunization requirements.
1. Measles/Mumps/Rubella.
Complete Option 1 or Option 2.
Option 1: Two doses of live MMR on or after the first birthday (Must have been given at least 28 days apart.)
Date #1
(mm-dd-yy) _______________________ Date #2 (mm-dd-yy) _______________________
Option 2: If vaccines were given separately, select one each for Measles, Mumps, and Rubella.
Measles. Check one box only.
Two doses of live vaccine administered on or after the first birthday (Must have been given at least 28 days apart.)
Date #1
(mm-dd-yy) ______________________ Date #2 (mm-dd-yy) _______________________
Physician-diagnosed illness Date (mm-dd-yy) _________________________
Protective antibody titer Date (mm-dd-yy) _________________________ Lab positive negative If negative, student must receive vaccine.
Mumps. Check one box only.
Two doses of live vaccine administered on or after the first birthday
Date #1
(mm-dd-yy) ______________________ Date #2 (mm-dd-yy) ______________________
Physician-diagnosed illness Date (mm-dd-yy) _________________________
Protective antibody titer Date (mm-dd-yy) _________________________ Result: positive negative If negative, student must receive vaccine.
Rubella. Check one box only. (Previous clinical diagnosis of rubella is not sufficient.)
One dose of live vaccine administered on or after the first birthday
Date
(mm-dd-yy) ________________________
Protective antibody titer Date (mm-dd-yy) _________________________ Result: positive negative If negative, student must receive vaccine.
2. Meningococcal Vaccine.
Check all that apply.
For any of the ACYW-135 (*) meningococcal vaccines, the date of your vaccine should be within the past 5 years.
Menactra™ * Date (mm-dd-yy) _______________________
Menveo™ * Date (mm-dd-yy) _______________________
Menomune™ * Date (mm-dd-yy) _______________________
Meningococcal ACYW-135 * Specify other brand or brand unknown ________________________________________________
Date (mm-dd-yy) _______________________
Trumenba™ (for Type B only) Date #1 (mm-dd-yy) _______________________ Date #2 (mm-dd-yy) ________________________ Date #3 (mm-dd-yy) ______________________
Bexsero™(for Type B only) Date #1 (mm-dd-yy) _______________________ Date #2 (mm-dd-yy) ________________________
I have decided not to obtain the meningococcal vaccine. I understand I must sign and upload Cornell Health’s Meningococcal Waiver Form.
[This form is available on the New Student Immunizations and TB History form (item #16) accessed through myCornellHealth.]
3. Tetanus/diphtheria/pertussis booster (Tdap) Date (mm-dd-yy) ________________________ You must have received a Tdap vaccine in the past 10 years.
4. Varicella (Chicken Pox). Check all that apply.
If you were born in the U.S. before 1980, this requirement does not apply.
Two doses of vaccine Date #1 (mm-dd-yy) ______________________ Date #2 (mm-dd-yy) ______________________
Physician-diagnosed illness Date (mm-dd-yy) _________________________
Protective antibody titer Date (mm-dd-yy) _________________________ Result: positive negative If negative, student must receive vaccine.

RECOMMENDED IMMUNIZATIONS
These immunizations are recommended by the U.S. Centers for Disease Control and Prevention (CDC) and the American College Health Association. To protect
your health, we urge students to receive these important vaccinations (or begin the series) before starting at Cornell. Please provide dates.
Hepatitis A Vaccine
Date #1 (mm-dd-yy) ___________________________ Date #2 (mm-dd-yy) ____________________________
Hepatitis B Vaccine
Date #1 (mm-dd-yy) ___________________________ Date #2 (mm-dd-yy) ____________________________ Date #3 (mm-dd-yy) ____________________________
HEP A / HEP B Combined Vaccine
Date #1
(mm-dd-yy) ___________________________ Date #2 (mm-dd-yy) ____________________________ Date #3 (mm-dd-yy) ____________________________
Human Papillomavirus (HPV) Vaccine Series (recommended for students of all genders, 26 and under)
Date #1
(mm-dd-yy) ___________________________ Date #2 (mm-dd-yy) ____________________________ Date #3 (mm-dd-yy) ____________________________
OTHER VACCINATIONS YOU MAY HAVE RECEIVED
HIB Vaccine (Haemophilus Influenza B) Date (mm-dd-yy) ______________________________
Pneumococcal Vaccine
Date (mm-dd-yy) __________________________
Polio Vaccine (before age 18) Check one box only.
IPOL Date of most recent dose (mm-dd-yy) _________________________
OPV Date of most recent dose (mm-dd-yy) _________________________
EPV DOSE #1 (mm-dd-yy) _________________________ DOSE #2 (mm-dd-yy) _________________________ DOSE #3 (mm-dd-yy) __________________
Rabies Vaccine
Date #1 (mm-dd-yy) ___________________________ RabAvert Imovax Unknown
Date #2
(mm-dd-yy) ___________________________ RabAvert Imovax Unknown
Date #3 (mm-dd-yy) ___________________________ RabAvert Imovax Unknown
Typhoid Vaccine Date (mm-dd-yy) __________________________
Yellow Fever Vaccine Date (mm-dd-yy) __________________________
TUBERCULIN (TB) SCREENING TEST
REQUIRED for full-time students from countries with a high incidence of TB: T-SPOT or Quantiferon-TB Gold blood test. Students with a positive result
must have a chest x-ray. If you are unable to get your required test before arriving at Cornell, you will have to get it as soon as you arrive.
Recommended for all students, especially those who have spent time in countries with a high incidence of TB.
Review list of countries with a high incidence of TB on the New Student Immunization and TB Screening History form at myCornellHealth.
Check all Tuberculin screening tests you have had.
PPD, Mantoux (skin tests) Date (mm-dd-yy) _________________________ Result: ____________ mm of induration
T-SPOT®.TB (blood test) Date (mm-dd-yy) _________________________ Result: positive negative
QuantiFERON®-TB Gold (blood test) Date (mm-dd-yy) _________________________ Result: positive negative
Chest x-ray Date (mm-dd-yy) _________________________ Result: normal abnormal
HEALTH CARE PROVIDER INFORMATION AND SIGNATURE
Signature Date (mm-dd-yy)
Name Work Phone
last, first, middle degree/title
Address

Tuberculosis (TB) Screening
COUNTRY LIST
Documentation of recent TB screening is:
• Required for students from “high incidence” countries (see World Health Organization list: www.who.int/tb/data/en)
• Recommended for all students, especially those who have lived or spent time in a country that has a “high incidence” of TB
Students from these countries are REQUIRED to submit documentation of recent TB screening due to HIGH INCIDENCE of TB.
Afghanistan
Aland
Islands
Algeria
Angola
Anguilla
Antarctica
Argentina
Armenia
Azerbaijan
Bangladesh
Belarus
Belize
Benin
Bhutan
Bolivia
Bosnia & Herzegovina
Botswana
Brazil
Brunei Darussalam
Bulgaria
Burkina Faso
Burundi
Cambodia
Cameroon
Canary Islan
ds
Cape Verde
Central African Republic
Chad
China
Columbia
Comoros
Congo
Congo DR
Cote d’Ivoire
Djibouti
Dominican Republic
Ecuador
El Salvador
Equatorial Guinea
Eritrea
Ethiopia
Fiji
French Guinea
Gabon
Gambia
Georgia
Ghana
Guam
Guatemala
Guernsey
Guinea
Guinea
-Bissau
Guyana
Haiti
Honduras
Hong Kong
India
Indonesia
Iraq
ISIR Profile Country
Isle of Man
Jersey
Kazakhstan
Kenya
Kiribati
Korea
-DPR
Korea
-Rep
Kosovo
Kuwait
Kyrgyzstan
Lao PDR
Latvia
Lesotho
Liberia
Lithuania
Macao
Madagascar
Malawi
Malaysia
Maldives
Mali
Marshall Islands
Mauritania
Mauritius
Mexico
Micronesia
Moldova
-Rep
Mongolia
Montenegro
Morocco
Mozambique
Myanmar
Namibia
Nauru
Nepal
New Caledonia
Nicaragua
Niger
Nigeria
Niue
Northern Mariana Islands
Pakistan
Palau
Panama
Papua
New Guinea
Paraguay
Peru
Philippines
Portugal
Qatar
Republic of Serbia
Romania
Russian Federation
Rwanda
Saint Barthé
lemy
Saint Martin
Saint Pierre and Miquelon
Saint Vincent & the Grenadines
Sao Tome & Principe
Saudi Arabia
Senegal
Serbia
Seychelles
Sierra Leone
Singapore
Sint Maarten
Solomon Islands
Somalia
South Africa
South Soudan
Spain
S. Georgia & S.
Sandwich Islands
Sri Lanka
Sudan
Suriname
Swaziland
Syrian Arab Republic
Taiwan
Tajikistan
Tanzania
-UR
Thailand
Timor
-Leste
Togo
Tokelau
Tonga
Tunisia
Turkmenistan
Tuvalu
Uganda
Ukraine
Uruguay
US Minor Outlying Islands
Uzbekistan
Vanuatu
Venezuela
Vietnam
Wallis & Futuna Islands
Yemen
Zambia
Zimbabwe
Students from these countries are NOT REQUIRED to submit documentation of recent TB screening due to LOW INCIDENCE of TB.
Albania
America Samoa
Andorra
Antigua and Barbuda
Aruba
Australia
Austria
Bahamas
Bahrain
Barbados
Belgium
Bermuda
Bouvet Island
British Indian Ocean Territory
British Virgin
Islands
Canada
Cayman Islands
Chile
Christmas Island
Cocos (Keeling) Islands
Cook Islands
Costa Rica
Croatia
Cuba
Curacao
Cyprus
Czech Republic
Denmark
Dominica
East Timor
Egypt
Estonia
Falkland Islands (Malvinas)
Faroe Islands
Finland
France
French
Polynesia
French Southern Territories
Germany
Gibraltar
Greece
Greenland
Grenada
Guadeloupe
Heard and McDonald Islands
Holy See (Vatican City State)
Hungary
Iceland
Iran
Ireland
Israel
Italy
Jamaica
Japan
Jordan
Lebanon
Libyan Arab Jamahiriya
Liechtenstein
Luxembourg
Macedonia
-TFYR
Malta
Martinique
Mayotte
Monaco
Montserrat
Netherlands
Netherlands Antilles
New Zealand
Norfolk Island
Northern Ireland
Norway
Oman
Palestinian Territory, Occupied
Pitcairn
Poland
Puerto Rico
Reunion
Saint Helena
Saint Kitts and
Nevis
Saint Lucia
Samoa
San Marino
Scotland
Slovakia
Slovenia
Svalbard and Jan Mayen
Sweden
Switzerland
Trinidad and Tobago
Turkey
Turks and Caicos Islands
United Arab Emirates
United Kingdom
United States of America
United States Virgin Islands
Wales
Western Sahara
West Bank & Gaza Strip
02/2018

Intercollegiate/NCAA athletes: Physical exam after March 1, 2018 is required. Sports Clearance Form must be completed by a health care provider and submitted with this form.
All other students: Physical exam within the past eighteen months is strongly recommended.
Student Name _____________________________________________________________________________________________ Date of Birth __________________________________
Date of physical exam
(mm-dd-yyyy) __________________________________________________________________________ Cornell net ID#
GENERAL MEDICAL INFORMATION
Height _______________________ Weight ________________________ Blood Pressure ________________________ Heart Rate _________________________
General Appearance __________________________________________________ Marfan stigmata Present Absent
Visual Acuity (Snellen, e.g., 20/40)
Uncorrected: Left Eye ______ / _______ Right Eye ______ / _______
Corrected: Left Eye ______ / _______ Right Eye ______ / _______
Check normal or abnormal for each item (comment below on all abnormal).
Normal Abnormal Normal Abnormal
• Eyes/Pupils • Pulses (simultaneous femoral and radial pulses)
• Mouth/Teeth • Heart (murmurs–auscultation standing, supine, +/- Valsalva)
• Neck/Thyroid • Skin (e.g., HSV, lesions suggestive of MRSA, tinea corporis)
• Lungs • Genitourinary (males only)
• Abdomen/Hernia
Musculoskeletal (Including ranges of motion, surgical scars, and anomalies) Check normal or abnormal for each item for athletes and students with orthopedic problems.
Normal Abnormal Normal Abnormal
• Ankles • Hands
• Back • Hips
• Elbows • Knees
• Feet • Neck
Comment on abnormal fi ndings. _______________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________
CLINICAL TESTS (required only for NCAA athletes)
Hemoglobin __________________________________________ OR Hematocrit ______________________
Sickle Cell Trait test result (NCAA athletes must provide a copy of the actual lab report) Negative Positive
Other relevant test results ______________________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________
ORGAN LOSS Evidence of a loss of any paired organ? Yes No Please specify ________________________________________________________________________
HISTORY OF HOSPITALIZATION OR SURGERY (INCLUDING ORTHOPEDIC)
Yes No If yes, please explain. ___________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________
Able to participate in all sports without restriction?
Yes No If no, please specify recommendations for physical activity. _______________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________
DOCUMENTATION Please provide records related to ongoing care (EKG's, MRIs, stress tests, etc.).
Current medical and mental health issues
_____________________________________________________________________________
_____________________________________________________________________________
_____________________________________________________________________________
Recommendations for continuing care
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
(fi rst, middle, last) (mm-dd-yyyy)
HEALTH CARE PROVIDER SIGNATURE
☛ Signature ___________________________________________________________________________________________________Date (mm-dd-yyyy) ________________________________
Name ___________________________________________________________________________________________________________Work Phone ____________________________________
(last, fi rst, middle) (degree/title)
Address _________________________________________________________________________________________________________________________________________________________
Normal Abnormal
• Shoulders
• Duck walk,
single leg hop
Physical Examination for Entering Students
See instructions for completing/returning this form on next page.
Instructions
1. Health care provider:
• Complete Physical Examination form in full.
• Provide signature and contact information.
• Attach copies of any appropriate documentation.
2. Student — return ONE COPY only:
• UPLOAD through myCornell Health: mycornellhealth.health.cornell.edu
– Log in with Cornell net ID, password, and date of birth.
– From Home Screen, click on “Messages.”
– Then “New message;” then “Send message or attachment to Health Records.”
– We accept the following fi le types: PNG, JPG, JPEG, GIF, PDF (no larger than 4 MB).
– Upload your physical exam form as one attachment and any supporting documentation in separate
attachments. If any document is more than one page, please upload as a single, multi-page attachment.
• or FAX: 607.255.0269
• or MAIL: Cornell Health Attn: Requirements Offi ce
110 Ho Plaza
Ithaca, NY 14853-3101
Instructions: RECRUITED INTERCOLLEGIATE/NCAA ATHLETE
1. Health care provider:
• Complete Physical Examination form in full.
• Complete Sports Clearance form in full (see below).
• For student athletes on medications for ADHD/ADD, complete "ADHD/ADD Medical Exception Form" (see below).
• Provide signature and contact information.
• Attach copies of any appropriate documentation (must include Sickle Cell Trait Lab report).
2. Student athlete — return ONE COPY only:
• UPLOAD through myCornell Health: mycornellhealth.health.cornell.edu
– Log in with Cornell net ID, password, and date of birth.
– From Home Screen, click on “Messages.”
– Then “New message;” then “Send message or attachment to Health Records.”
– We accept the following fi le types: PNG, JPG, JPEG, GIF, PDF (no larger than 4 MB).
– Upload your physical exam form as one attachment, your sports clearance form as a separate attachment,
and any supporting documentation as separate attachments. If any document is more than one page, please
upload as a single, multi-page attachment.
• or FAX: 607.255.0269
• or MAIL: Cornell Health Attn: Requirements Offi ce
2
